
Want to Age Well? Hit These Strength Targets: Longevity-Based Strength Standards
Key Points:
Muscular strength is one of the strongest predictors of longevity. Higher total-body strength is linked to lower mortality, reduced risk of chronic disease, and better long-term independence.
Grip strength alone underestimates true functional capacity. Compound lifts like squats, deadlifts, and rows provide a more complete picture of total-body strength and coordination.
Verro’s strength standards use estimated 1RMs (e1RMs) scaled to bodyweight. This makes the targets fair, functional, and applicable across all body types and fitness levels.
The standards are evidence-based and age-adjusted. They incorporate research on sex and age-related muscle decline to keep expectations realistic and sustainable.
e1RM strength reflects healthspan, not just performance. These metrics focus on strength that supports mobility, independence, and disease prevention throughout life.
Introduction: Why e1RM Strength Standards Matter for Longevity
Strength training isn’t just about performance or aesthetics—it’s increasingly recognized as one of the most powerful tools we have for improving healthspan, reducing risk of chronic disease, and maintaining independence with age. Numerous studies have shown that muscular strength is a strong predictor of longevity in both men and women across a wide range of ages.
For instance, handgrip strength alone has been repeatedly shown to predict all-cause mortality, cardiovascular disease, and disability (Bohannon, 2008; Leong et al., 2015). However, grip strength is a proxy for total-body strength—and likely underestimates the importance of compound strength patterns like squats, deadlifts, and pulls that engage large muscle groups and require neuromuscular coordination.
Thus, rather than relying on grip strength alone, Verro has charted our strength standards around the concept of estimated one-repetition maximums (e1RMs) for key movement patterns, scaled to bodyweight. This better reflects total-body strength relevant for functional aging.
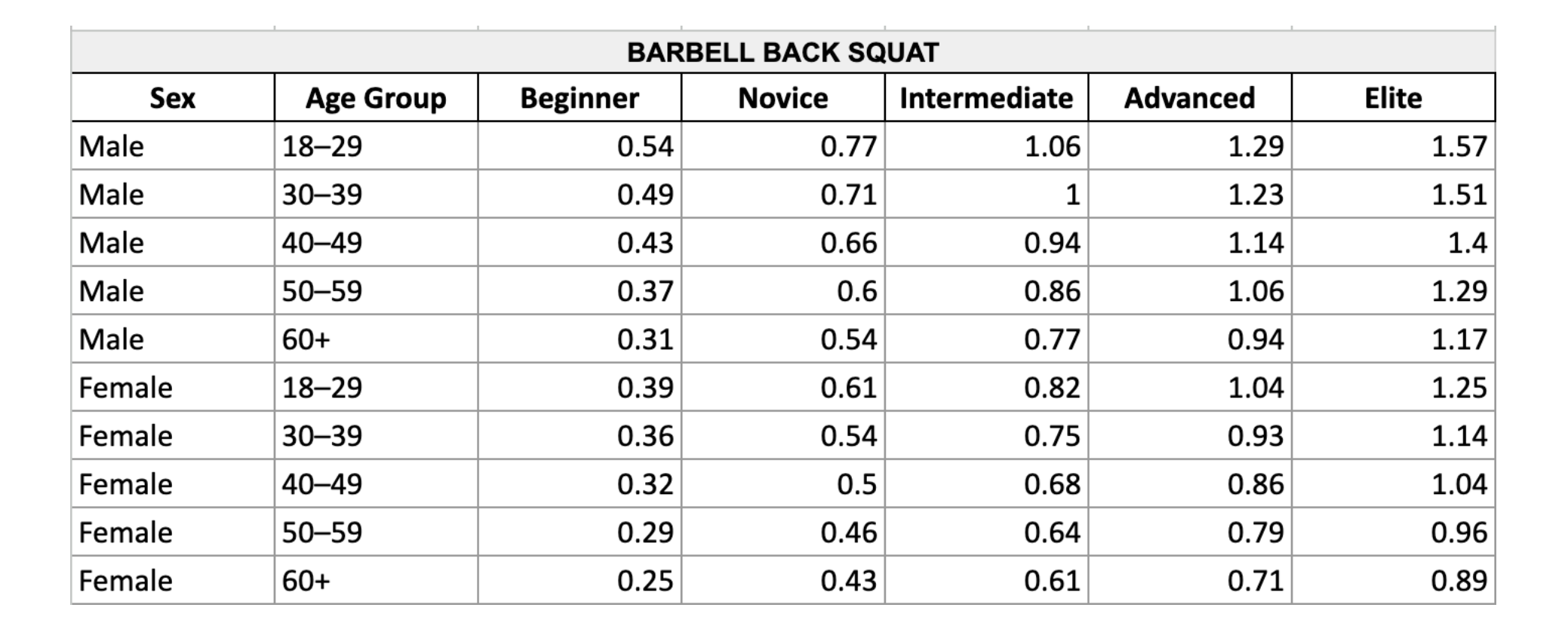
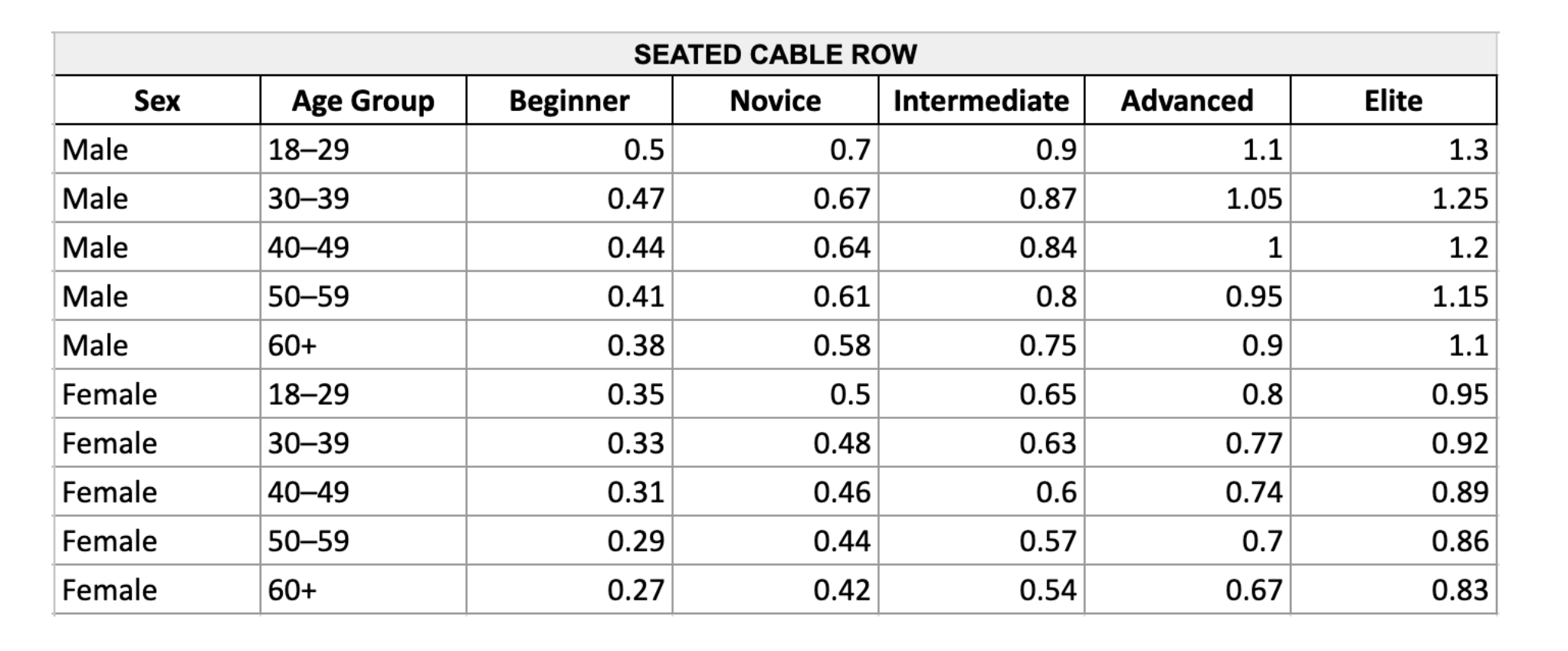
For the purposes of this article, I used barbell back squat, barbell bench press, lat pulldown, trap bar deadlift, seated db overhead press, and seated row as examples, but you could use other exercises from the same family (pullups instead of pulldowns, leg press instead of squat, etc.), but for the purposes of this article I thought it would be good to include just one example from each of the fundamental movement patterns.
Strength Standards
Each e1RM standard in the chart is expressed as a multiple of your bodyweight. For example, if the standard for a trap bar deadlift is 1.75× bodyweight and you weigh 160 pounds, your target would be a 280-pound deadlift. This approach makes the standards scalable, fair, and applicable across a wide variety of body sizes and compositions. By framing strength relative to body mass, we focus on functional strength—not just absolute numbers.




Methodology: How the Numbers Were Derived
These e1RM standards were reverse-engineered based on three principles:
Sufficient Muscle and Strength for Health Benefits
Scaled Resistance Relative to Body Mass
Sustainable Load Across the Lifespan
For each of the six movements (squat, hinge, vertical push, vertical pull, horizontal push, horizontal pull) five tiers were defined: beginner, novice, intermediate, advanced, and elite
These levels are scaled by age and sex using known trends in strength capacity decline and muscle mass reduction with age (Mitchell et al., 2012; Goodpaster et al., 2006). For example, the natural loss of muscle mass (sarcopenia) starts as early as age 30 and accelerates beyond 60. Therefore, standards decline slightly each decade to remain attainable without unrealistic expectations.
Where applicable, ratios were guided by population averages found in data from:
National Strength and Conditioning Association (NSCA)
StrengthLevel.com databases
Scientific literature on age and sex-based muscular performance
For instance, research by Fragala et al. (2019) emphasizes the value of using relative strength (to body mass) to assess long-term health and functional independence, especially in aging adults. These charts follow that advice.
Why These Standards Correlate with Longevity
1. Reduced Risk of Mortality and Morbidity
Higher muscular strength is consistently linked to lower all-cause mortality, particularly when measured as relative strength (Volaklis et al., 2015). Even moderate improvements in strength can significantly reduce the risk of death from cardiovascular events, cancer, and respiratory diseases (Ruiz et al., 2008).
2. Improved Metabolic and Cardiovascular Health
Resistance training improves insulin sensitivity, blood pressure, and lipid profiles (Strasser et al., 2012). Stronger individuals often have healthier body composition and lower levels of visceral fat—both predictors of metabolic syndrome.
3. Prevention of Disability and Fall Risk
Strength, especially in lower-body and postural muscles, directly reduces the risk of falls, frailty, and mobility loss (Landi et al., 2012). Exercises like squats and deadlifts are critical for maintaining the ability to get up from a chair, climb stairs, or recover balance.
4. Preservation of Muscle Mass and Bone Density
Mechanical loading through compound movements preserves lean body mass and bone mineral density, helping to prevent osteoporosis and sarcopenia, which are major drivers of aging-related decline (Watson et al., 2018).
Why Use e1RM?
Estimated 1RMs provide a clear, standardized way to assess maximum strength capacity without requiring maximal effort tests. They're more scalable and safer for older populations or those training with longevity in mind. The use of e1RM also aligns with recent research showing that high-effort sets at low volume can be as effective for strength as traditional high-volume work, especially when using velocity-based training and RPE scales (Schoenfeld et al., 2021). To see the e1rm calculator we use at Verro, check out this article.
Conclusion: A Scalable, Functional Standard for Strength and Aging
These e1RM standards aren’t just performance metrics, they represent durable, achievable, and meaningful strength benchmarks for individuals interested in staying strong and independent throughout life. They are not elite powerlifting targets or CrossFit benchmarks, they are targets that align with healthspan, function, and disease prevention. We hope you find them useful.
References
Bohannon, R. W. (2008). Hand-grip dynamometry predicts future outcomes in aging adults. J Geriatr Phys Ther, 31(1), 3–10.
Fragala, M. S., et al. (2019). Resistance training for older adults: Position statement from the National Strength and Conditioning Association. J Strength Cond Res, 33(8), 2019–2052.
Goodpaster, B. H., et al. (2006). The loss of skeletal muscle strength, mass, and quality in older adults: The Health, Aging and Body Composition Study. J Gerontol A Biol Sci Med Sci, 61(10), 1059–1064.
Landi, F., et al. (2012). Sarcopenia and mortality among older nursing home residents. J Am Med Dir Assoc, 13(2), 121–126.
Leong, D. P., et al. (2015). Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet, 386(9990), 266–273.
Mitchell, W. K., et al. (2012). Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol, 3, 260.
Ruiz, J. R., et al. (2008). Muscular strength and adiposity as predictors of adulthood cancer mortality in men. Cancer Epidemiol Biomarkers Prev, 17(11), 3723–3729.
Schoenfeld, B. J., et al. (2021). Resistance training volume enhances muscle hypertrophy but not strength in trained men. Med Sci Sports Exerc, 53(3), 456–463.
Strasser, B., et al. (2012). Resistance training in the treatment of the metabolic syndrome. Sports Med, 42(5), 365–381.
Volaklis, K. A., et al. (2015). Muscular strength as a strong predictor of mortality in health and disease. J Musculoskelet Neuronal Interact, 15(4), 365–377.
Watson, S. L., et al. (2018). Resistance training volume and bone mineral density in adults: A systematic review. Osteoporosis International, 29(3), 561–571.
DISCLAIMER
This article is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider or certified fitness professional before starting any new training program, especially if you have any pre-existing health conditions or injuries. Individual results may vary, and adjustments to training volume, exercise selection, and intensity should be made based on your personal recovery capacity, experience level, and goals.
Other Blogs On Data & Research







